
Context
Role
User researcher with service design focus
Team
1-2 user researchers, 1 service designer
Client
UK Teaching Hospital Foundation Trust
Phase
Discovery
Timeline
8 months
Ownership
Delivered 17 journey blueprints; built most of 5; research informed 13 in total.
Note
Due to NDA constraints, the organisation name has been anonymised and original deliverables are not shown.
Summary
The problem
A hospital foundation trust needed to migrate to a modern electronic patient registration system, but their processes had never been properly documented—most of the knowledge lived in people’s heads.
The risk
Realistically, if a department like A&E all got on a plane and it crashed, those processes would go with them.
What we did
To address this, we documented how care actually works by doing on-the-ground research next to healthcare workers, supported by interviews and system walkthroughs.
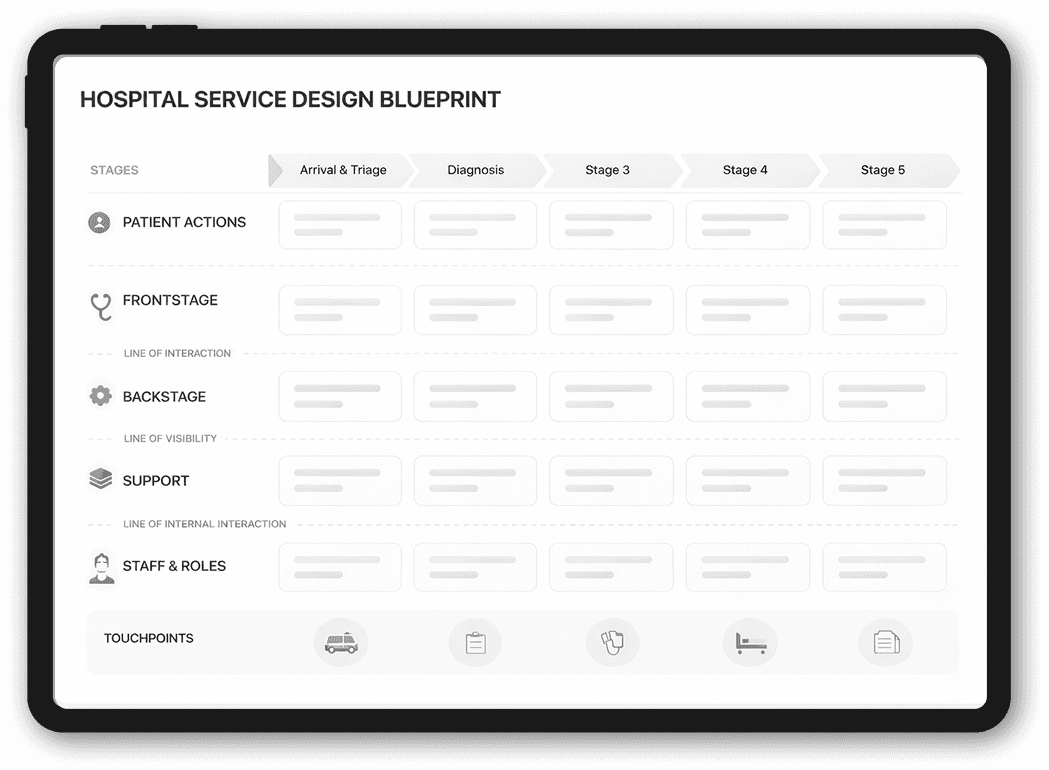
What we produced
We brought everything together into service blueprints, process maps, user journeys, and personas that teams can use day to day.
The result
We mapped how care actually works, documented previously informal processes, and identified practical improvements to reduce risk ahead of the EPR migration.

The challenge
Hospital processes live in people, not in systems
The trust was preparing to migrate to a new electronic patient record (EPR) system, but existing processes were inconsistent, often undocumented, and varied across departments.
Much of the work relied on informal practices and individual knowledge, making it hard to build a shared understanding of how care was delivered.
It was also important to identify inefficiencies early, so they wouldn’t be carried into the new system.
Our approach
We worked alongside those delivering care
Observations
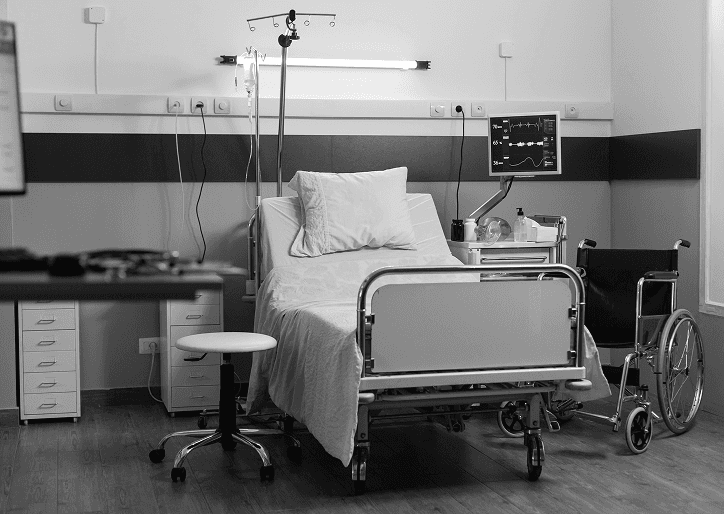
We went straight to the source: hospital wards and the emergency department.
We observed staff in their day-to-day work to understand real workflows, complemented by in-depth interviews and system walkthroughs.
Deliverables
We translated these insights into practical outputs:
High-level blueprints of care delivery
Level 2 process maps of roles and responsibilities
User journeys and personas
Research reports summarising key insights
Extra steps to organise and make sense of the information
To help make everything more usable, we also introduced a few additional tools and ways of working:
Pain point tracker
We created a simple spreadsheet to organise pain points by role, theme, department, and phase. This made it much easier to filter insights depending on what needed to be designed.
Calling out complex ecosystems
Hospital processes are rarely linear—they often contain smaller ecosystems within them (like referrals or blood testing). When we came across these, we highlighted them in the research reports, as they needed their own deeper dive and mapping.
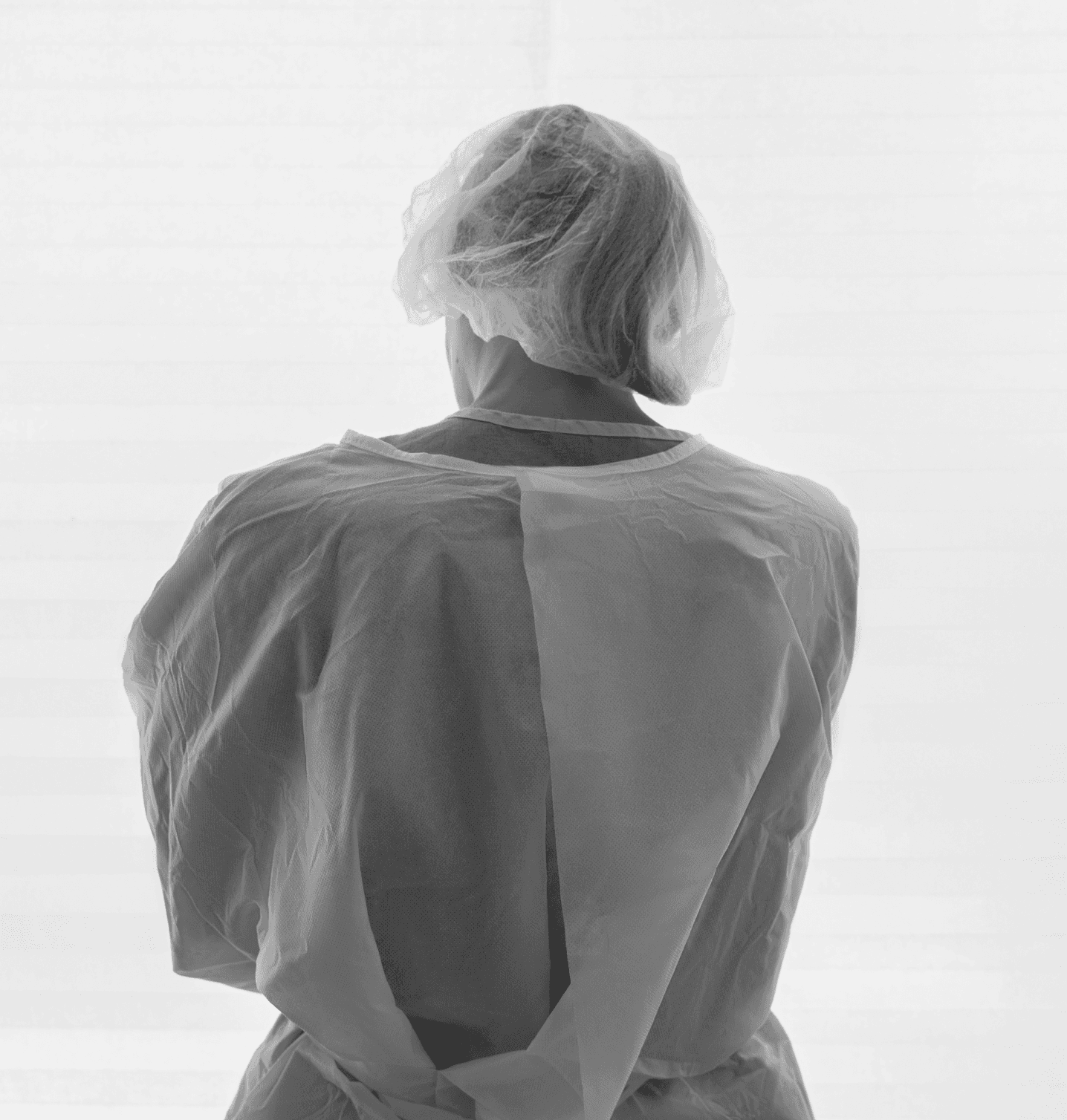
Keeping the human side visible
It’s a long way from the bottom to the top, and by the time insights reach decision-makers, the deeply human side of hospital work can get flattened into business decisions. We used strong quotes and storytelling in our reports and presentations to keep the heart of the work visible.

Insights
The system did not always reflect reality
The current system doesn’t reflect what actually happens on the wards. As a result, it often gets in the way of healthcare workers. And when every minute counts, this can even become dangerous:


Pain points
Inconsistent frailty scoring
The frailty score helps guide care for more vulnerable patients. Staff are not consistently capturing the frailty score, which means decisions are often based on age rather than actual need. As a result, patients aren’t always guided to the right place at the right time, early opportunities for support are missed, and delays build up later in their care journey.
Unclear patient schedule
Patients are added to a long list in the ward planner, but it’s not clear who is coming in, when they’re arriving, or what they need.This makes planning difficult, leading to scheduling conflicts, delays, and unnecessary visits for patients, while also increasing reliance on paper-based workarounds.
Proforma doesn’t fit therapist work
The current system doesn’t fit how therapists actually work. The proforma assumes every A&E patient needs a full assessment, when in reality therapists focus on the specific problem. It’s also too rigid, requiring fields like mobility even when they’re not relevant (e.g. a broken arm), with no way to mark them as not applicable. Because of this, therapists work around it—skipping parts or documenting in their own way to keep things moving.
Unclear patient journey
Using multiple systems alongside paper leads to workarounds and inconsistent ways of working. The patient’s journey ends up feeling fragmented, and it’s hard to piece together what happened, when, and who was involved.
Care and system out of sync
The system doesn’t reflect how care actually happens. Staff prioritise treating patients first and often update the system later, which means records can appear incomplete or overdue. This creates a gap between what’s happening in reality and what’s shown in the system, sometimes making it seem like care hasn’t been delivered when it has.
Recommendations
Use frailty scoring
Make the frailty score part of how triage already works, so it’s captured as a natural step rather than an extra task. Give staff simple guidance and support so they feel confident using it, and add light prompts in the system to help it be recorded consistently.
Design for scannability
Make the ward planner easier to scan and actually plan from. Instead of one long list, show patients by time and include key details about what they need. Adding simple columns or tags—like P/E or DVT reviews—would help staff quickly understand what’s coming in and prioritise.
Perform an audit
Audit and rework the therapy proforma to better support how therapists assess patients in A&E. Make fields like mobility more flexible by allowing them to be marked as not applicable, and shift from full assessments to more problem-focused documentation.
Reflect the patient journey
Bring patient information together in one place. This should show a clear view of the patient’s journey—where they’ve been (e.g. A&E → AMU → ward) and who did what at each step. This makes it easier to understand what’s happened and make informed decisions.
Outcomes
A shared understanding and a path foward
Over 8 months, this work built a shared understanding of care delivery and enabled more confident decision-making.
Aligned teams around real-world care delivery
Processes that were previously informal and inconsistent are now documented and accessible across teams.
Reduced risk ahead of the EPR migration
Dependencies and variations are now visible, helping teams anticipate and address issues earlier.
Turned complex pain points into prioritised action
Key pain points were translated into concrete recommendations, making it easier to prioritise what to change.
Established a baseline for continuous improvement
Instead of starting from scratch, teams now have a baseline that can evolve over time.
Stronger stakeholder engagement with storytelling
Framing the insights through real examples helped stakeholders connect with the problems and created urgency to act.

Reflections
A few key learnings and limitations stood out
Learnings
EPRs should be shaped where care happens
Without observing work on the ward, key parts of care are not visible, which can lead to systems that block rather than support staff.
Issues often arise at handovers
When responsibility or information moves between people or stages, things become less clear and workarounds appear.
Trust takes time in clinical environments
Staff are often interrupted and can be guarded, so being clear about intent and anonymity is essential.
Creating space builds trust
Giving staff space to share their experiences helps build trust and surface important insights.
Hospitals are made up of interconnected ecosystems
Multiple overlapping systems exist within hospitals. It is important to identify them early and decide where to focus.
Limitations
Research in hospitals comes with practical constraints
An outbreak of a stomach virus meant we had to move between wards, and an A&E relocation required us to adapt our research plans.
We were brought in too late to influence key decisions
The hospital had already chosen a new EPR system before fully understanding the existing landscape, limiting how much impact our research could have.
Stakeholder alignment isn’t always achievable
Despite strong internal relationships, we lacked a consistent connection with the new EPR team, limiting our influence—so we created a filterable Excel to make it easy to find relevant insights
